
501-500-5105
Male, Case 1
Male, Case 1
Male, Case 1
"I feel like I can not breathe in and out of my nose and always breathe through my mouth."
Consult Appointment
Consult Appointment
Working Diagnosis
Working Diagnosis
Comprehensive Records
Comprehensive Records
Treatment Plan Presentation
Treatment Plan Presentation
Consult Appointment:
Consult Appointment:
- Patient presented with a chief complaint of: chronic mouth breathing, morning time headaches, feels like mouth is too small
- Medical/Dental history reviewed: 28 y.o. patient has a history of asthma and controls with inhaler as needed. Patient also reported a history of prior orthodontics where he had four permanent teeth removed. Limited other dental history. Patient was not currently taking any medications.
- Doctor spent time talking about TMD, facial growth, and the different cause and effects to the patient
- Clinical Exam: Doctor performed zero base exam which consists of palpating the patient's head and neck muscles, opening and closing evaluation, dental exam, and myofunctional assessment
- Working Diagnosis: after exam, doctor gave patient his initial impressions of the case and the degree of difficulty. A general idea of treatment was presented. To confirm these initial assumptions, the doctor needs comprehensive records
- These records can be taken on the same day as consult or rescheduled depending on patient preference.
Working Diagnosis:
The working diagnosis is based off the doctors initial exam and results from the consult appointment. This is subject to change after records, but is utilized to give patient a general idea of what their treatment could look like.
The working diagnosis from this patient was the following:
- Nasomacillary Complex
- Retruded mandible: lower jaw sits further back than ideal and has a steep angle on the jaw line (see pictures to follow)
- Poor Tongue posture: Tongue sits in the floor of the mouth instead of pressed against the palate
- Chronic Mouth Breather
- Postural Airway compensation: Patient has small airway and holds head and neck in a way to maximize the airway. Usually forward and rotated head posture.
Comprehensive Records:
After the consult appointment, this patient agreed to go forward with comprehensive records. These records include:
- EMG Muscle Readings: Computerized Jaw Tracking
- Pictures: Intra-oral (teeth) and extra-oral (face)
- CBCT: Scan of head and neck area for pathology scan and TMJ evaluation
- Digital Impressions: Scan of the teeth and the bite for lab to construct necessary appliances
- Eccopharyngometry: Measurement of airway space
- Any other records doctor deems necessary for patient's case
- These records were then used to form a treatment plan specific to the patient
Treatment Plan Presentation:
- The following information show pictures from the records appointment as well as a screenshot from the patient's CBCT
- These pictures are marked up to illustrate some findings that are obtained during the treatment planning process
- The doctor will go over these findings and the treatment plan either in-office or over the phone with the patient
- After hearing the treatment plan and official diagnosis from the Doctor, this patient agreed to go forward with Phase one of treatment

Nasomacillary Complex or Midface:
Nasomacillary Complex or Midface:
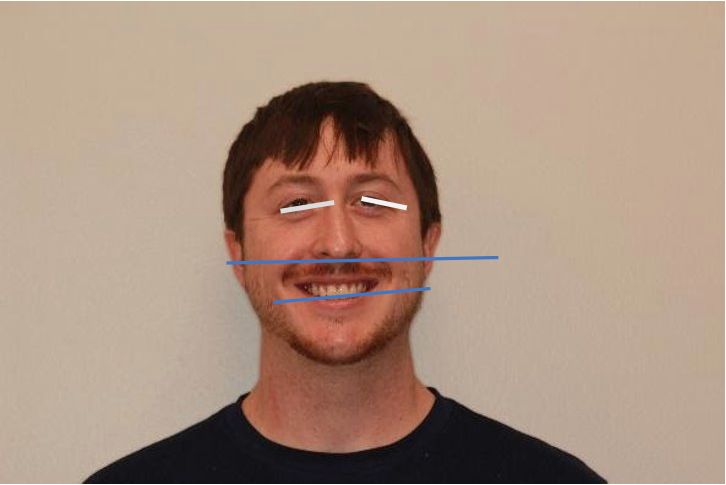
- The middle and lower thirds of the face should approximate a 1:1 relationship. However, as you can see from the brackets, the lower third is longer than the middle third.
- Mouth Breathing
- Cause: Evolution, diet, nursing habits, genetics
- Effects: low nasal volume, mouth breathing, limited room for upper teeth, altered mandibular development (lower jaw)
Underdeveloped Nasomaxilla or Midface:
Underdeveloped Nasomaxilla or Midface:
- Downward slanting canthus: lack of development of the midface leaves the lower bony border of the eye socket undersized and thus gives the appearance of downward slanted eyes.
- Canted Upper arch: patient is underdeveloped and had an altered growth vector. The patient experienced excessive vertical growth.
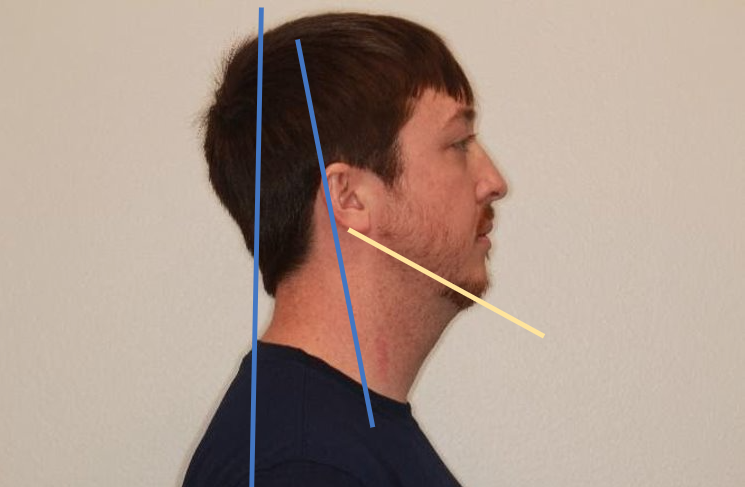
Signs of Forward Head Posture:
Signs of Forward Head Posture:
- Ears in front of the shoulders
Signs of Rotated Head Posture:
- Usually in conjunction with forward head posture
- Head rotated slightly backwards
Cause:
- This is the body's result of obtaining the best airway possible. The body's number one requirement is oxygen. So, if oxygen is hard to obtain, it will change many things including the position we hold our heads in to get oxygen easier.
Effects:
- Chronically fatigued neck and back of head muscles. Open mouth posture. Altered whole body posture.
High Mandibular Plane Angle:
High Mandibular Plane Angle:
Translation:
- The lower jaw angle from the profile view is slanted towards the floor instead of more parallel with the floor
Cause:
- Altered growth direction of the mandible due to the chronic mouth breathing and tongue resting in floor of mouth
Effects:
- Increases airway volume in lower portion of airway which makes it easier to breathe through the mouth
- Poor facial esthetics
- Long lower third of face

Narrow Arch Form:
Narrow Arch Form:
Cause:
- Lack of development in the upper arch which led to crowded upper teeth
- Prior orthodontics removed two teeth from each arch which shrinks the size of the arches down
Effects:
- "black triangles" when the patient smiles
- Not considered esthetically pleasing
- Lack of room for soft tissue like the TONGUE
- Promotes open mouth posture to keep tongue from being forced back in to airway
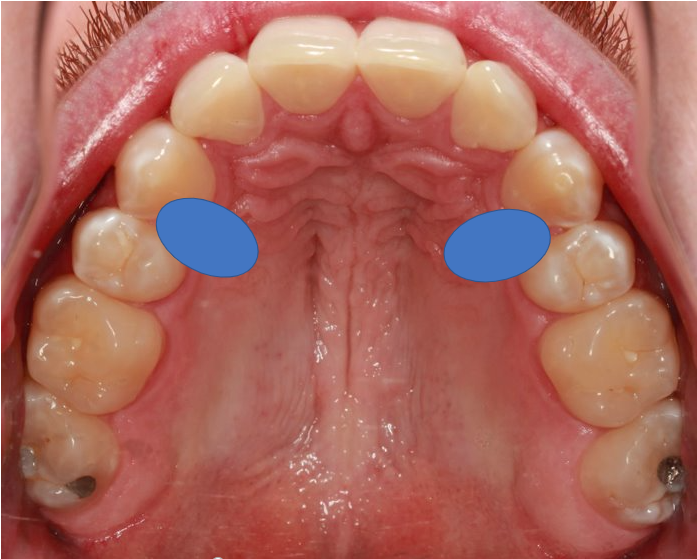
Missing Premolars:
Missing Premolars:
Cause:
- Patient has had prior orthodontics to straighten teeth.
- To make space, the prior orthodontist removed teeth in order to straighten the remaining teeth
Effect:
- Reduced arch space
- No room for tongue to be in proper position
- Open mouth breathing posture to keep tongue from blocking airway
- Black triangles

"Dumped" Lower Molars
"Dumped" Lower Molars
Cause:
- Tongue rests in the floor of mouth due to chronic mouth breathing
- Posterior teeth tip in towards the tongue
Effect:
- Locked bite: upper teeth lock in the lower teeth when patient bites together
- Lateral movements of lower teeth come with grinding or rubbing against the upper teeth
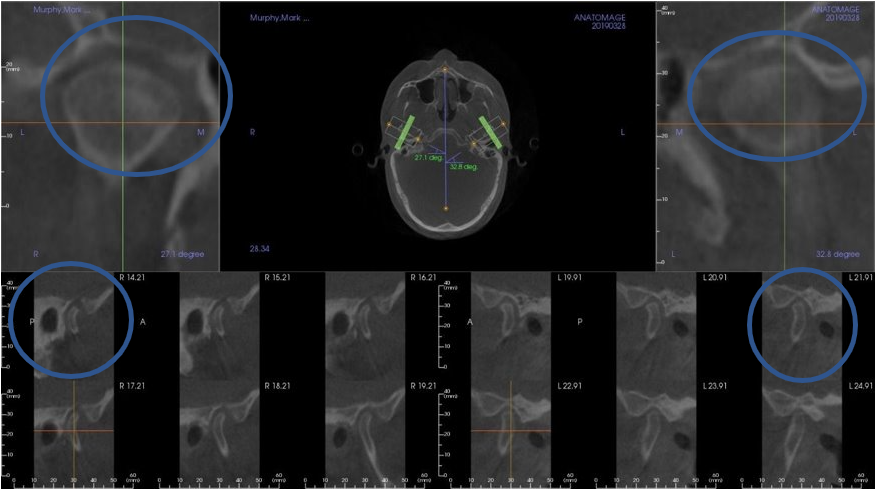
TMJ Findings from the CBCT:
TMJ Findings from the CBCT:
Right TMJ Findings:
- Upper Right Circle: Uniform vertical space from medial to lateral
- Lower Right Circle: Lower jaw (condyle) is near the back of the joint space, close to the earhole
- Mild arthritic changes to the bones of the jaw
Left TMJ Findings:
- Upper Left Circle: Vertical space diminishes towards the lateral part of this joint space
- Lower Left Circle: Head of lower jaw is changing shapes - "Beaking"
- Lower Left Circle: Lower jaw is near back of joint space, close to earhole
VISIT
12400 Cantrell Road, Suite 1LIttle Rock, Arkansas 72223
CONTACT
(P)501-500-5105(F) 501302-2925dandzdental@gmail.com
CONNECT
symmetrylr.com ©2019 | A DealFamilyDental.com
Company